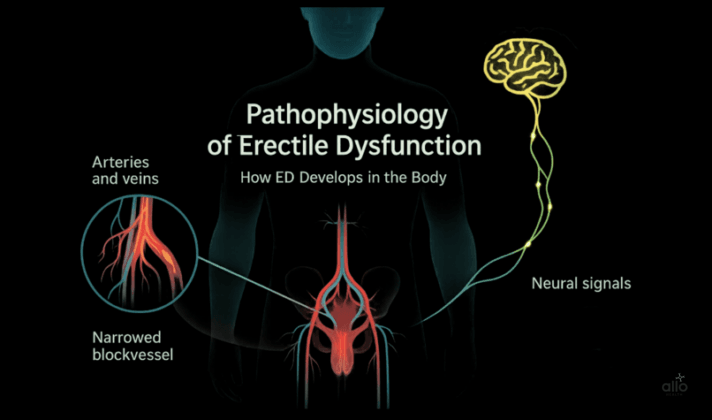
Pathophysiology of Erectile Dysfunction: How ED Develops in the Body
Written by Dr. Pranitha Bangera

Dr. Pranitha Bangera is a gold-medalist healthcare professional with an elite foundation in clinical training and patient care. A researcher at heart, she specializes in creating high-impact, research-driven medical content that empowers readers through accessible patient education. Dr. Bangera focuses on the intersection of digital health and clinical communication, specifically within the fields of sexual health and mental well-being. Her work is dedicated to making complex medical innovations understandable and trustworthy for a global audience.
•
April 15, 2026
Our experts continually monitor the health and wellness space, and we update our articles when new information becomes available.
Quick Read
Erectile dysfunction happens when the normal process of arousal, brain signals, nerve activity, blood flow, and hormone support, breaks down. If blood doesn’t fill the penile chambers, nerves don’t carry signals properly, or the balance of chemical messengers is disrupted, erections become weak or inconsistent. Understanding this chain of events, known as the pathophysiology of ED, helps explain why different treatments work for different men.
Erectile dysfunction (ED) means having trouble getting or keeping an erection firm enough for sex. It’s very common in men. More than just a sexual concern, ED can affect self-confidence, relationships, and even signal health issues like diabetes mellitus, heart disease, or broader cardiovascular disease. In this article, we’ll look at how erections normally happen, what goes wrong in the body, and why this knowledge is key to understanding and treating ED.
Allo asks
What Do You Think Causes Most Cases of ED?
What Does Pathophysiology Really Mean?
“Pathophysiology” may sound like a heavy medical term, but it simply refers to how and why a health issue develops inside the body. If physiology explains how things normally work, pathophysiology explains what happens when things go wrong. ED is much more common than most men realize. Studies estimate that around 30–40% of men in their 40s and over 50% of men above 50 experience some degree of erectile difficulties. [1]
How a Normal Erection Works (The Physiology)
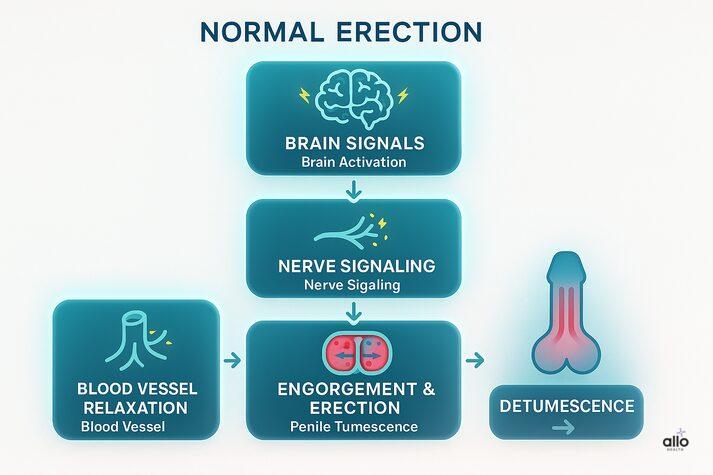
Before diving into what goes wrong, let's first look at how an erection normally happens — covering ED ke lakshan alongside helps connect symptoms to this physiology. Think of an erection as a team project where the brain, nerves, blood flow, hormones, and penile structures work together. The process happens in the following order: Brain Signals (Brain Activation) ↓ Nerve Signaling ↓ Blood Vessel Relaxation ↓ Engorgement & Erection (Penile Tumescence) ↓ Losing the erection (Penile Detumescence)
1. Brain Signals (Brain Activation)
Sexual desire starts in the brain. Thoughts, emotions, or touch trigger the neurovascular events. The brain sends impulses down the spinal cord (including nuclei such as Onuf's nucleus) to the penis area (pelvis).
2. Nerve Signaling
Upon receiving signals from the brain, nerves in the penis release nitric oxide (NO), a chemical messenger — erect meaning in Hindi explains this process in accessible terms. NO then activates cyclic GMP (cGMP) inside muscles of the penis (cavernous smooth muscle).

3. Blood Vessel Relaxation
Now the cGMP helps with the blood vessel relaxation. What is cGMP? It is a tiny molecule inside cells that works like a “switch.” It tells the smooth muscle around the penile blood vessels to relax. This relaxation opens the arteries wider, allowing more blood flow into the penis. At the same time, it also helps veins close off, trapping blood inside and creating a firm erection. This allows more blood to flow into two sponge-like chambers in the penis called the corpora cavernosa.
4. Engorgement & Erection (Penile Tumescence)
The tunica albuginea is a tough, fibrous outer layer that surrounds the corpora cavernosa (the main erectile chambers in the penis). Think of it like a strong elastic sleeve. When the penile erectile tissue fills with blood during arousal, the tunica albuginea stretches and compresses the veins that normally drain blood out. This “trapping effect” keeps blood inside the penis, increases penile rigidity, and maintains the erectile response until “detumescence”.
5. Losing the erection (Penile Detumescence)
Detumescence is the process of “losing an erection.” After orgasm (also ejaculation) or when stimulation stops, the chemical signals fade, blood flows out, and the penis returns to its resting state. When everything is in sync, erections feel natural and dependable. But if even one part of this chain breaks down, ED can occur.
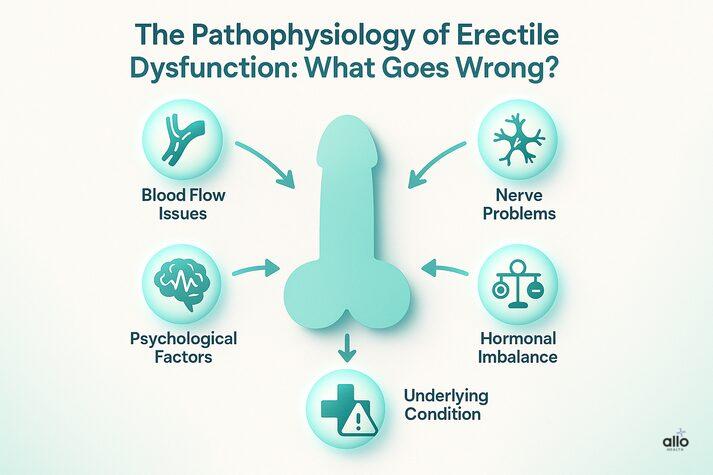
Erectile Dysfunction Pathophysiology: What Goes Wrong?
ED develops when:
- Blood can’t flow properly
- Nerve signals don’t reach the penis
- Hormones fall out of balance
- The mind blocks arousal
- There’s an underlying condition.
Let’s look at each of these pathways to understand how things can go wrong inside the body.

1) Vascular Problems (Blood Flow Issues)
One of the most common culprits behind ED is poor blood flow. For a normal erection, the arteries need to open wide to let blood rush in, and the veins need to hold it there until sex is over. If either part of this system doesn’t work properly, whether blood can’t get in or leaks out too quickly, ED can happen. Many cases of erectile dysfunction can be traced back to issues with blood vessels (vascular diseases). This type of ED is known as vascular erectile dysfunction. This can happen due to:
- Narrowing of Arteries: Some health conditions (atherosclerosis and metabolic syndrome) can make the arteries that supply blood to the penis harder and narrower. With less blood able to flow in, erections may feel weaker or fade too quickly.
- Venous leak: Sometimes the problem isn’t getting blood into the penis, but keeping it there. If the veins don’t close tightly enough, blood can escape too quickly. This venous leakage (venogenic erectile dysfunction) makes it hard to stay firm, even if an erection starts normally.
- Endothelial dysfunction: The endothelium is the thin lining inside blood vessels that helps them relax and open by releasing a chemical called nitric oxide. When conditions like smoking, diabetes, or high blood pressure damage this lining, it can’t do its job properly. Without that relaxation signal, blood flow to the penis is reduced, making erections more difficult.
Why does this matter? Because ED diagnosis and tests rely precisely on understanding where in this pathway things break down. Studies show that ED often appears years before heart disease symptoms. In fact, men with ED are more likely to develop cardiovascular disease later. [2] This makes ED an important early warning sign for overall vascular health. Common conditions that can cause blood vessel (vascular) problems linked to ED:
- High blood pressure (hypertension)
- Diabetes
- High cholesterol
- Heart disease and Atherosclerosis
- Obesity
- Smoking
- Sedentary lifestyle
2) Neurological Problems (Nerve Pathways)
Erections start with a signal from the brain that travels down the spinal cord and into the nerves of the penis. If these nerves are damaged, the message may not get through. Without clear nerve signals, the body struggles to trigger or maintain an erection. Common causes of damage include:
- Neuropathy from diabetes: High blood sugar damages nerves, making it harder for signals to travel. Research shows that up to 50–75% of men with long-term diabetes experience ED. [3]
- Spinal cord injuries: Block of nerve impulses, especially if the injury is in the lower back.
- Neurological conditions: Diseases like Parkinson’s or multiple sclerosis interfere with brain–nerve signaling, reducing erectile function. [4]
- Pelvic surgeries: Procedures for prostate or bladder cancer (radical prostatectomy) can unintentionally damage nerves and impair erectile response.
3) Hormonal Imbalances
Hormones act like messengers that keep sexual desire and function on track. If these levels are too low or out of balance, it can reduce interest in sex and make erections more difficult. [5] Some of these hormones are:
- Testosterone: Often called the “male hormone,” testosterone fuels sexual desire and supports erectile function. Low testosterone due to health conditions (hypogonadism or hypogonadotropic hypogonadism) can make it harder to feel interested in sex and to maintain erections.
- Thyroid disorders: Your thyroid controls energy and metabolism. When it’s overactive (hyperthyroidism) or underactive (hypothyroidism), it can disturb hormone balance and sometimes lower testosterone levels or cause mood and energy changes.
- High prolactin: Extra amounts of this hormone, sometimes caused by problems in the pituitary gland, can lower testosterone levels and affect erections.
- High cortisol: This “stress hormone” rises with chronic stress, which can interfere with blood flow and sexual performance.
4. Psychological & Emotional Factors
The mind is just as important as the body in sexual health. Stress, anxiety, depression, or relationship issues can block arousal signals before they even reach the body. Sometimes, the fear of not getting an erection becomes the very reason it doesn’t happen and creates a frustrating cycle. Common psychological causes of ED include:
- Stress & anxiety: Worrying about performance, work, or personal issues can block brain signals needed for arousal.
- Depression: Low mood and energy affect both desire and physical response.
- Relationship issues: Lack of communication or emotional distance from a partner can make erections harder to achieve.
Psychological factors can sometimes cause “situational ED.” In this case, a man may still get normal erections during sleep or while masturbating, but has trouble maintaining one during sex with a partner.
5) Metabolic Factors
Diabetes is one of the strongest risk factors for erectile dysfunction. Research shows that up to three out of four men with diabetes mellitus experience ED at some point.[6] Diabetes mellitus exerts a “triple hit” on erectile function by disrupting three key systems:
- Blood vessels: High blood sugar damages the inner lining of arteries (vascular endothelium), making it harder to release nitric oxide. Over time, this reduces circulation.
- Nerves: Diabetes can injure the nerves that carry signals from the brain to the penis (a problem called diabetic neuropathy).
- Hormone and metabolism changes: Insulin resistance and long-term inflammation can stiffen arteries and make it harder for blood to flow(vascular resistance).
6) Oxidative Stress and Inflammation
Another key factor behind ED is oxidative stress. This can happen when too many harmful molecules, called reactive oxygen species (ROS), build up in the body. These molecules block nitric oxide (NO). Without enough nitric oxide, blood vessels stay tight, circulation drops, and inflammation rises, all of which make erections harder. Oxidative stress also triggers the RhoA/ROCK pathway(RhoA/Rho kinase pathway), which acts like a “brake pedal” on the smooth muscles of the penis. [7] When this pathway is overactive, the muscles stay too tight and blood can’t flow in properly. Together, low nitric oxide and an overactive RhoA/ROCK pathway create a double barrier, making it even more difficult to achieve or maintain an erection.
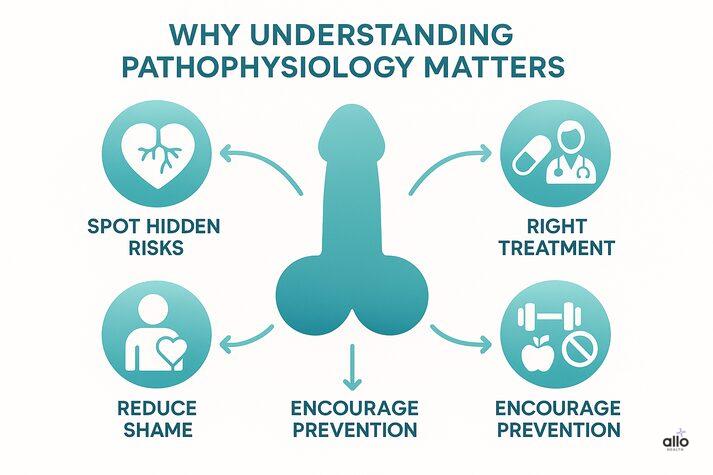
Why Understanding Pathophysiology Matters in Erectile Dysfunction
By looking at how ED develops, we uncover several important insights.
- ED can act as an early warning sign of hidden health risks like cardiovascular disease, diabetes, or high blood pressure. It also helps doctors (and patients) choose the right treatment, whether that’s medication to improve blood flow, therapy for stress, or hormone replacement for imbalances.
- Just as importantly, knowing that ED often arises from a mix of physical and emotional factors reduces shame, helping men realize it’s not their fault.
- Finally, this understanding encourages prevention: lifestyle changes such as exercise, eating well, quitting smoking, and managing chronic conditions improve not only heart health but also sexual health.
This knowledge directly guides treatment — which is why consulting the right doctor for ED is essential for an accurate diagnosis.
- Diagnosis often begins with a medical history, physical exam, and blood tests for glucose, lipids, testosterone, thyroid, or prolactin levels.
- Questionnaires like the International Index of Erectile Function and functional tests such as nocturnal penile tumescence monitoring or Doppler ultrasound can help pinpoint whether the cause is vascular, neurological, or hormonal.
- Once the root cause is identified, treatments can be matched more precisely.
Treatment Options Include:
- Lifestyle and Preventive Care: Regular exercise, a balanced diet, avoiding smoking and excess alcohol, and controlling conditions like diabetes or high blood pressure can make a significant difference.
- Medications (First-Line): PDE-5 inhibitors (sildenafil, tadalafil, vardenafil) enhance nitric oxide pathways to relax blood vessels. They’re effective if nerves and vessels are intact, though less so in advanced vascular or nerve damage cases.
- Devices and Local Treatments: Options include vacuum erection devices, constriction rings, penile injections, intraurethral suppositories, penile rehabilitation after surgery, and even low-intensity shockwave therapy to stimulate new blood vessel growth.
- Surgical Options: Penile implants (prostheses) provide reliable erections when other approaches fail.
- Hormone Therapy: Testosterone replacement or correction of thyroid/prolactin imbalances can restore sexual function in men with hormone-related ED.
- Psychological and Relationship Support: Counseling or sex therapy addresses performance anxiety, stress, or relationship challenges, often working best alongside medical treatments.
“Understanding the pathophysiology of ED helps us take away the shame. When you see it’s a medical condition with real causes, it becomes clear that it’s treatable and not your fault.”
Conclusion
By looking at the pathophysiology of ED, we see how blood flow, nerve signals, hormones, and the mind all play a role in healthy erections. When one or more of these systems breaks down, ED can appear as an early warning sign of deeper health concerns like diabetes or heart disease. The good news is that ED is treatable. Understanding why it happens makes it easier to find the right treatment. Whether from lifestyle modifications and PDE-5 inhibitors to penile injections, vacuum erection devices, shockwave therapy, and penile implants, care can be tailored to the cause. Most importantly, no one should feel ashamed to seek help.

Disclaimer
The following blog article provides general information and insights on various topics. However, it is important to note that the information presented is not intended as professional advice in any specific field or area. The content of this blog is for general educational and informational purposes only. The content should not be interpreted as endorsement, recommendation, or guarantee of any product, service, or information mentioned. Readers are solely responsible for the decisions and actions they take based on the information provided in this blog. It is essential to exercise individual judgment, critical thinking, and personal responsibility when applying or implementing any information or suggestions discussed in the blog.
Most Asked Questions
What does “pathophysiology of erectile dysfunction” mean?
It simply means how ED develops inside the body. It explains the biological changes that cause erection problems.
Is erectile dysfunction mainly a blood flow problem?
Not always. Poor circulation is common, but ED can also come from nerve damage, hormone imbalances, or psychological stress. Often, it’s a mix of these factors.
Can stress alone cause ED?
Yes. Even if the body is healthy, stress or performance anxiety can block signals from the brain to the penis, leading to temporary ED.
Why is ED linked to heart disease and diabetes?
The same blood vessel problems that affect the heart and circulation also affect the penis. That’s why ED can sometimes be an early warning sign of other health issues.
If pills like Viagra don’t work, does that mean nothing will help?
Not at all. Pills work best when nerves and blood vessels are healthy. If they don’t help, other treatments like injections, pumps, therapy, or surgery may still be effective.
Sources
- 1.
Aging related erectile dysfunction—potential mechanism to halt or delay its onset
- 2.
Does erectile dysfunction predict cardiovascular risk?
- 3.
Prevalence of erectile dysfunction and associated factors among diabetic men
- 4.
Management of sexual dysfunction in Parkinson’s disease
- 5.
Hormonal Causes of Male Sexual Dysfunctions and Their Management
- 6.
Diabetes and Erectile Dysfunction
- 7.
RhoA/ROCK pathway inhibitor ameliorates erectile dysfunction